
Diagnosis to treatment of breast cancer
June 28, 2025
Has Your Fatty Liver Entered a Dangerous Stage Without You Knowing?
January 15, 2026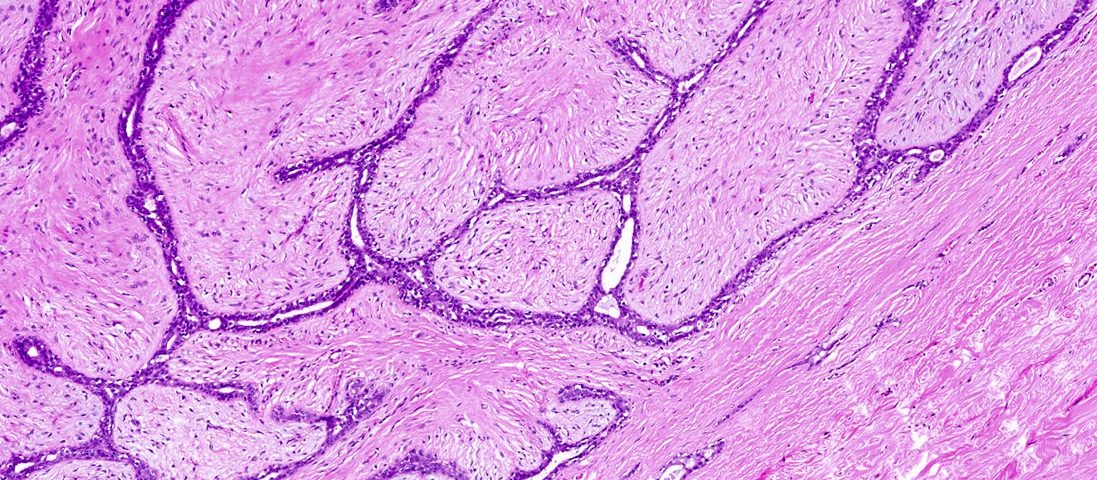
Fibroadenoma is the most common benign breast tumor, which affects predominantly young women, mostly between the ages of 15 and 35 years. They are made up of glandular tissue and breast connective tissue. Knowledge of the nature of these tumors, their presentation, investigation methods, and management to treat and reassure the patient is worthwhile. This article is a review of fibroadenomas from genuine sources.
- Types of fibroadenomas
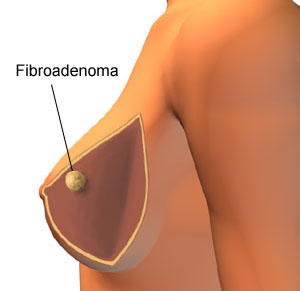
Fibroadenomas are solid, benign tumors with a sharp and distinct edge. They are usually round or oval in their form and firm or rubbery and mobile upon palpation (“a lump that slips beneath the fingers”). They may be as small as under one centimeter or as large as several centimeters and may enlarge or shrink over time, especially with the action of pregnancy hormones or hormone therapy.
Types of fibroadenoma
Simple Fibroadenoma:
This type is the most common. Under the microscope, they appear uniform and are not associated with an increased risk of breast cancer.
Complex Fibroadenoma:
This subtype is characterized by characteristics such as giant cysts (macrocysts – cysts that do not require the use of a microscope), calcifications (calcifications – calcium), adenosis (adenosis – formation of additional lobules), or papillary apocrine hyperplasia (papillary apocrine hyperplasia – change in lining cells). The existence of a complex fibroadenoma has the potential to be associated with an elevation of the risk of later breast cancer, but the risk is low and requires that it be monitored more closely.
Juvenile Fibroadenoma:
This type is found in girls and young women, typically between the ages of 10 and 18. It grows fast and sometimes very large but is never malignant.
Giant Fibroadenoma:
They are also referred to as fibroadenomas measuring larger than 5 centimeters in width or occupying a lot of breast tissue. They may require surgery to be removed.
(Tubular Adenoma):
A rare variety that is largely made up of glandular tissue.

Symptoms and signs of a fibroadenoma
- Lump: The most common symptom is the feeling of a round, firm, or rubbery mass with distinct edges in the breast. This lump is freely movable under the skin.
- Painless: Fibroadenomas are typically not painful. Tenderness or soreness can sometimes be experienced by some women, especially on the eve of menstruation, likely due to hormonal variations.
- . Change in size: The lump may change in size during the menstrual cycle or during pregnancy and breastfeeding (usually it grows). It may also grow, shrink, or even disappear without appearing to have any reason.
- Lack of other symptoms: Fibroadenomas are normally not accompanied by nipple discharge, skin dimpling, or nipple skin changes. The presence of these symptoms necessitates a prompt medical checkup.
Causes and risk factors of fibroadenoma
The exact etiology of the formation of fibroadenomas is unknown, but it seems that reproductive hormones, especially estrogen, play an important role in their formation.
Hormonal Factors: These masses usually happen in reproductive age, may grow in size during pregnancy or with administration of hormonal medicines such as hormone replacement therapy (HRT), and after menopause, with a reduction in the secretion of hormones, generally diminish or become static.
Age: Females aged 15 to 35 years have the highest risk of acquiring it, but they can acquire it at any age.
Family history: A history in the family of fibroadenoma may increase a person’s risk slightly.
Use of contraceptive pills before age 20: Some studies have shown that the use of contraceptive pills in the teen years can be associated with a small increase in risk for getting fibroadenomas.
Diagnosis of fibroadenoma
The diagnosis of a fibroadenoma requires clinical evaluations and imaging. The main objective is to confirm the benign nature of the mass and to rule out other lesions, especially breast cancer.
Clinical breast examination:
The doctor examines the size, shape, texture, and mobility of the lump by touching the breasts and underarm areas.
Filming:
- Diagnostic Mammogram: In females over 30 years or with some features, fibroadenoma may present as a round or oval smooth-margin mass on mammogram. Calcifications may be seen in complex ones.
- Breast Ultrasound: The initial-line diagnostic device in young women (age younger than 30 years) or women with dense breasts. Ultrasound is readily able to show the density of the mass, the normal shape, well-circumscribed border, and benign characteristics, making it distinct from a fluid-filled cyst.
Biopsy:
The only sure way of confirming that the mass is benign and determining the type of fibroadenoma (simple or complex). Routine practices are:
- Core Needle Biopsy: Optimal choice. Under ultrasound guidance and with a comparably dense needle, minor tissue samples from the mass are excised to be examined under a microscope by a pathologist.
- Fine-Needle Aspiration (FNA): The mass is aspirated of cells with an exceedingly fine needle. Though useful at times, the sample is often suboptimal or not to be trusted to rule out malignancy, so core biopsy is generally the better option.
- Excisional Biopsy: The entire mass is removed in a simple surgical procedure in this method. This method is generally used when less invasive biopsy methods (e.g., core biopsy) did not yield decisive results.
- Excisional Biopsy: In this technique, the whole mass is excised in a minor surgery. This technique is generally adopted if less invasive biopsy techniques (e.g., core biopsy) have proven indecisive or if the mass is too small and inaccessible.
Treatment and management of fibroadenoma
The. Choice of the best course of treatment depends on several factors, including the size and type of mass (simple or complex), the elicited symptoms (e.g., discomfort, pain), patient’s age, past medical and family history, patient’s concerns, and physician’s perception.
Active Monitoring / Watchful Waiting
This is the most common treatment method for tiny, non-symptomatic fibroadenomas with benign confirmation by biopsy. Since fibroadenomas do not pose a risk of cancer and could shrink or remain stable spontaneously, medical excision is not immediately necessary. The follow-up protocol normally includes:
- Physician physical exam every 6 months initially and then every year if the mass remains the same.
- Regular ultrasound of the breast (e.g., every 6 to 12 months) to monitor changes in size or shape of the mass.
- Mammography as a screening measure according to the patient’s age guidelines for screening.
Surgery: Excision of fibroadenoma may be recommended in the following cases:
- The mass is large or has been increasing rapidly.
- The mass has been responsible for causing pain, discomfort, or deformation of the breast.
- The results of the biopsy or imaging were inconclusive or raised concerns (for example, in complex fibroadenomas with unusual features).
The mass does not disappear on its own or remains large even after menopause.
- Severe patient concerns despite reassurance of benignity.
Types of surgery:
- Lumpectomy or wide local excision: Removal of the fibroadenoma with a thin margin of the overlying normal tissue.
- Enucleation: Removal of the mass of the fibroadenoma alone through dissection from the surrounding tissue. The method is usually used for discrete and benign masses.
- Minimally invasive methods: Some newer operations, such as vacuum-assisted excision via ultrasound guidance, may be utilized in small fibroadenomas.
Destruction by cryoablation (Cryoablation):
This process is done under local anesthetic and ultrasonography. Thin catheter is inserted into the center of the fibroadenoma, and with extremely cold gas (most commonly argon), the mass tissue is frozen and annihilated. As time passes (several months to a year), the dead tissue is slowly reabsorbed by the body. This process is suitable for small, well-defined fibroadenomas and causes a minimal scar.
Symptom management
For fibroadenomas that cause mild discomfort, especially cyclic tenderness related to menstruation, the following measures may be recommended:
- Use of a supportive bra.
- Limiting caffeine and salt intake (effective in some women).
- Use over-the-counter pain relievers such as acetaminophen or ibuprofen if needed.
- Warm or cold compress.
Conclusion
Breast fibroadenoma is very common benign breast tumor of young women.
Lumps are usually non-painful, mobile, and well-defined. Final diagnosis is with clinical examination, imaging (mammography or ultrasound), and often biopsy (more often core biopsy). Most fibroadenomas, especially simple and small ones, do not require surgical removal and can be safely managed with active follow-up (periodic examination and imaging). Operation or procedures such as cryoablation is reserved for symptomatic, large, rapidly growing, or suspicious (complex) masses primarily. Being aware that fibroadenomas are benign and are mostly dealt with without invasive procedure can go a long way towards soothing the patients. Follow-up, but also adherence to breast cancer screening programs by all women regardless of having or not having fibroadenomas, is still required.
{kind=link}